 A diagnosis of breast cancer raises immediate questions about treatment choices and their likely impact. Chemotherapy is a systemic therapy used in many situations; it circulates throughout the body to target cancer cells that may have spread beyond the original tumour. Chemotherapy can be given before surgery (neoadjuvant) to shrink tumours, after surgery (adjuvant) to reduce the risk of recurrence, or as a primary treatment for advanced disease. The drugs used and the intended goal of treatment vary according to cancer type, stage and individual patient factors. This guide explains how breast cancer chemotherapy works, outlines common regimens, describes typical side effects and practical management strategies, and highlights sources of support to help patients and their families make informed decisions.
A diagnosis of breast cancer raises immediate questions about treatment choices and their likely impact. Chemotherapy is a systemic therapy used in many situations; it circulates throughout the body to target cancer cells that may have spread beyond the original tumour. Chemotherapy can be given before surgery (neoadjuvant) to shrink tumours, after surgery (adjuvant) to reduce the risk of recurrence, or as a primary treatment for advanced disease. The drugs used and the intended goal of treatment vary according to cancer type, stage and individual patient factors. This guide explains how breast cancer chemotherapy works, outlines common regimens, describes typical side effects and practical management strategies, and highlights sources of support to help patients and their families make informed decisions.What Is Breast Cancer Chemotherapy and How Does It Work
Chemotherapy is a systemic cancer treatment delivered through the bloodstream so drugs reach the whole body. Unlike local treatments such as surgery or radiotherapy, systemic therapy can target cancer cells that have spread beyond the original tumour site.
These medicines act by disrupting cell division and growth. Because cancer cells typically divide more rapidly than normal cells, they are more vulnerable to agents that damage DNA or interfere with the proteins required for cell replication, leading to cancer cell death.
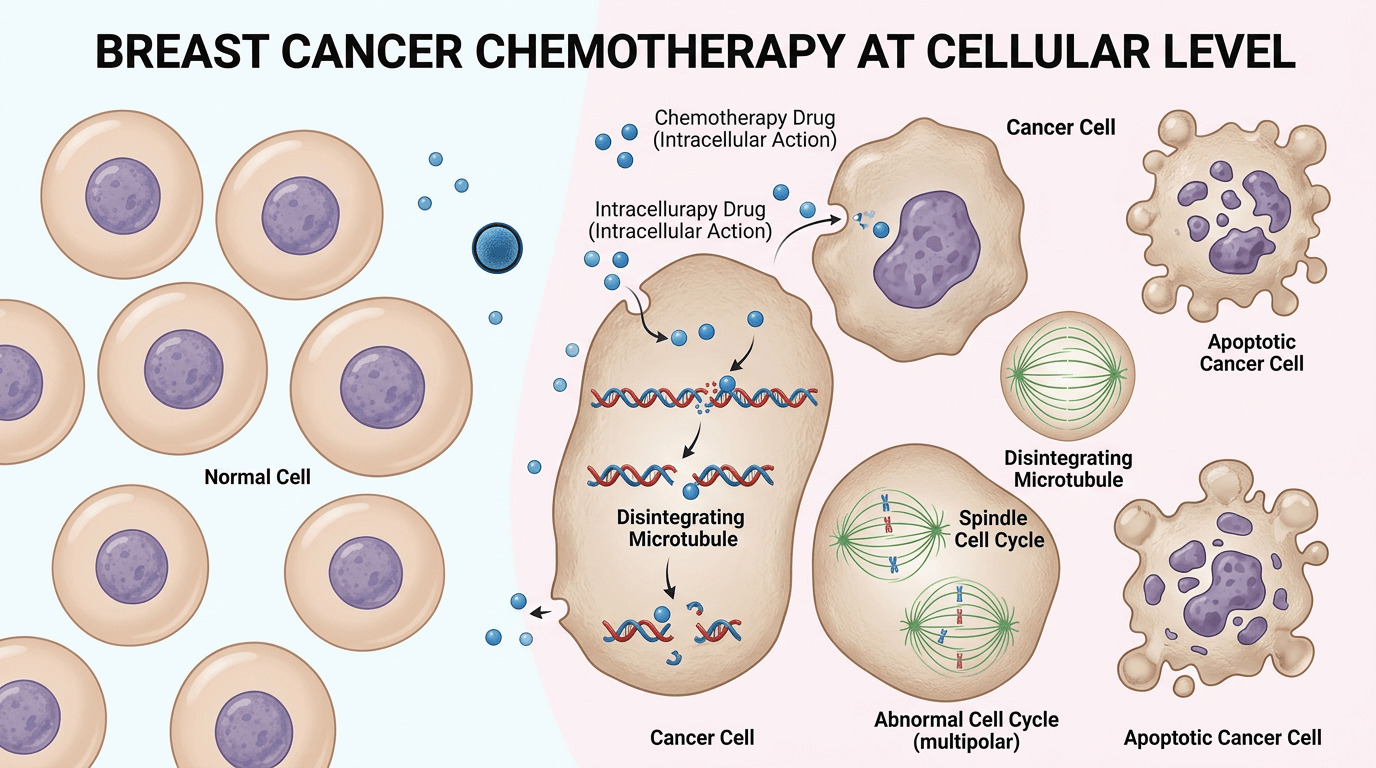 Different drugs act at different points in the cell cycle: some are most active while cells are dividing, others affect cells regardless of the phase. For this reason, combinations of drugs are commonly used to increase the chance of destroying cancer cells at multiple stages of growth and to reduce the likelihood of resistance.
Different drugs act at different points in the cell cycle: some are most active while cells are dividing, others affect cells regardless of the phase. For this reason, combinations of drugs are commonly used to increase the chance of destroying cancer cells at multiple stages of growth and to reduce the likelihood of resistance.
The treatment team selects chemotherapy agents according to tumour biology and the individual patient. Key factors include breast cancer subtype, stage, hormone receptor and HER2 status, lymph node involvement and the person’s age, general health and prior treatments.
Important Note: Modern chemotherapy protocols are increasingly personalised. Advances in genomic tests and other diagnostics help oncologists identify which patients are most likely to benefit, thereby avoiding unnecessary treatment and minimising side effects.
Types of Breast Cancer Chemotherapy and Their Purposes
Chemotherapy is used at different points in the care pathway, and its role depends on timing relative to other treatments. Each approach—before surgery, after surgery, or for advanced disease—has a distinct objective within the overall treatment plan.
Neoadjuvant Chemotherapy Before Surgery
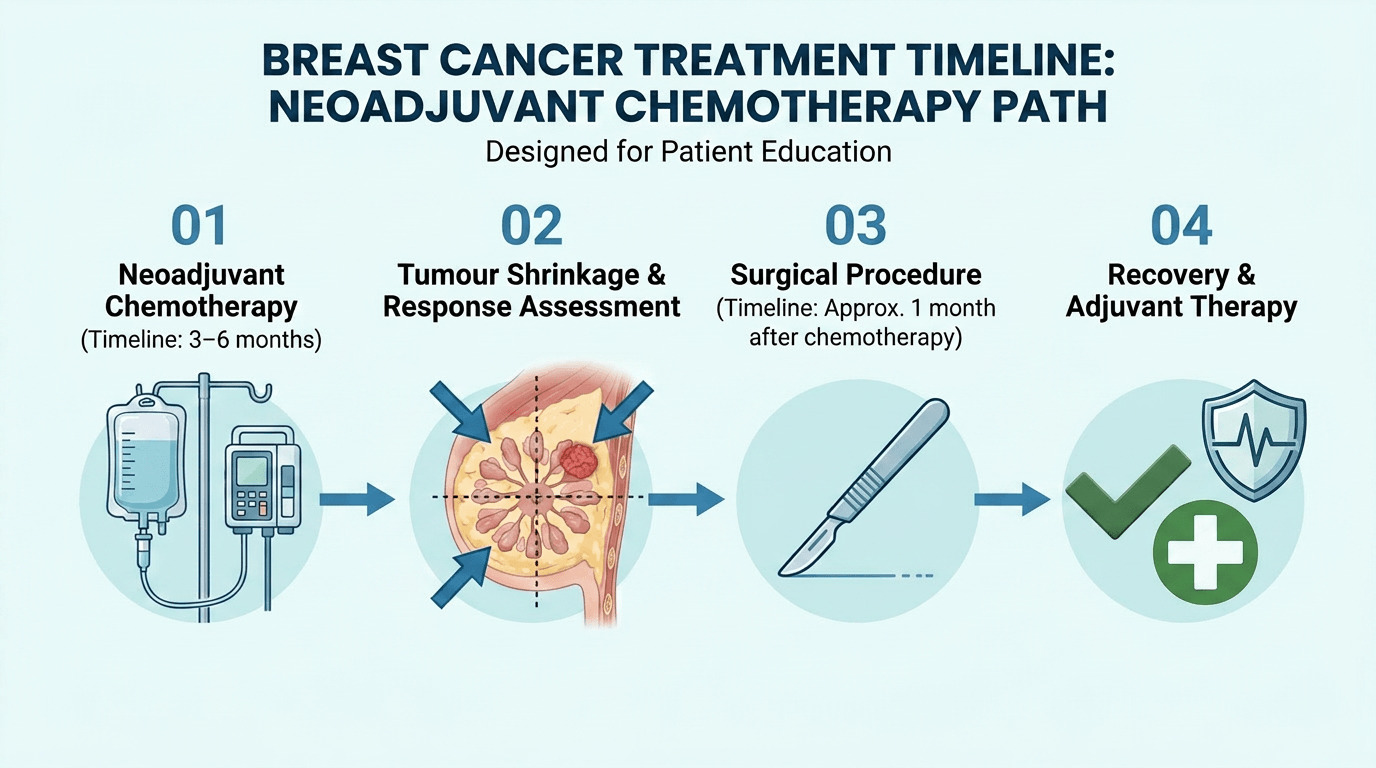
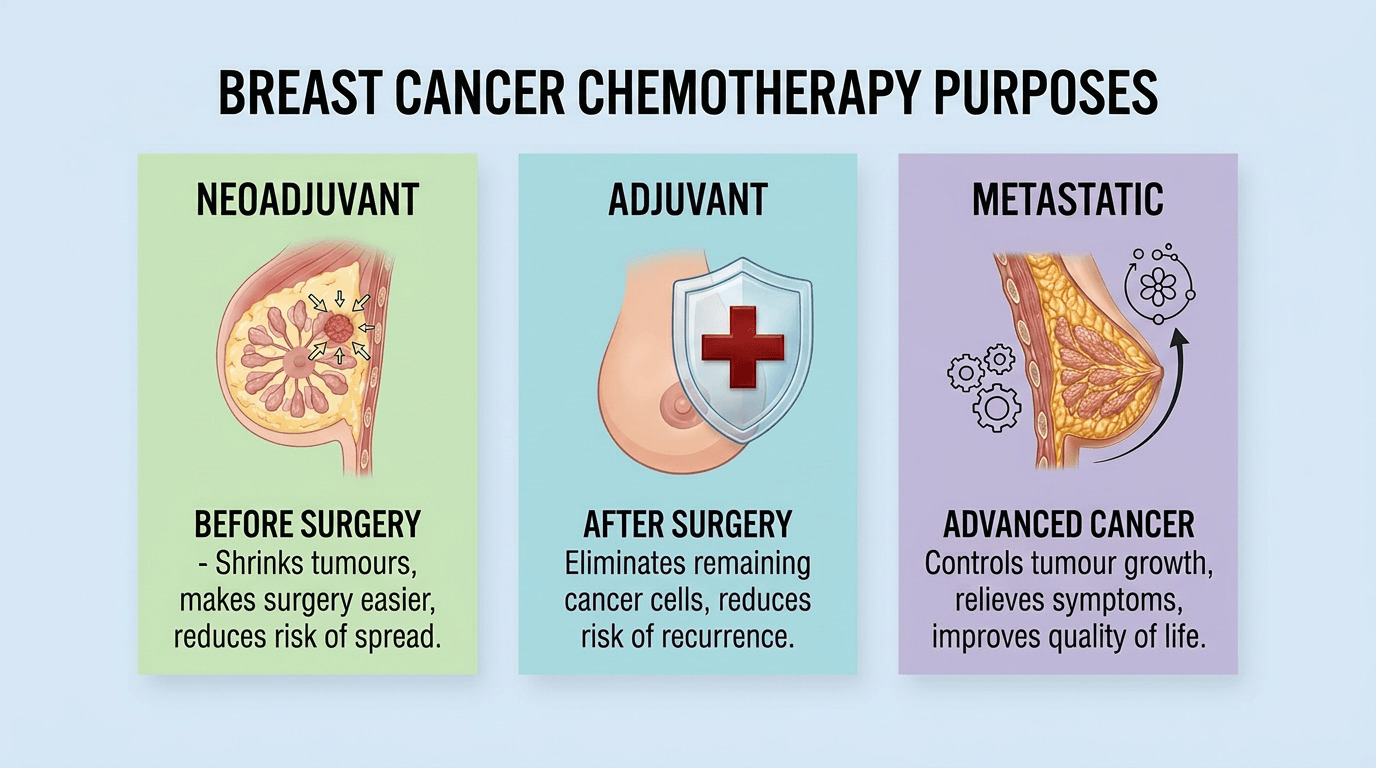
Neoadjuvant therapy is given prior to surgery to reduce tumour size and make surgical removal easier. In some cases, this can allow breast-conserving surgery (lumpectomy) instead of mastectomy.
This approach is particularly valuable for locally advanced or inflammatory breast cancer and for certain subtypes that respond well to systemic treatment. Treating before surgery also gives clinicians real‑time information about tumour sensitivity to the chosen drugs, which can guide post‑operative treatment decisions.
 Neoadjuvant therapy is now commonly used for triple‑negative and HER2‑positive breast cancers because these subtypes often show substantial shrinkage before surgery. Achieving a complete pathological response—no remaining cancer cells at the time of surgery—is associated with better long‑term outcomes.
Neoadjuvant therapy is now commonly used for triple‑negative and HER2‑positive breast cancers because these subtypes often show substantial shrinkage before surgery. Achieving a complete pathological response—no remaining cancer cells at the time of surgery—is associated with better long‑term outcomes.
Adjuvant Chemotherapy After Surgery
Adjuvant chemotherapy is given after surgery to eradicate microscopic cancer cells that might remain in the body despite complete removal of the visible tumour. The aim is to reduce the risk of recurrence.
The recommendation for adjuvant treatment depends on tumour size, lymph node involvement, grade and molecular features. Oncologists use a combination of clinical judgement, pathology and predictive tools to estimate recurrence risk and the likely benefit from chemotherapy.
Not every patient requires adjuvant chemotherapy. People with very small, early‑stage, hormone receptor positive tumours may be effectively managed with endocrine therapy alone. Genomic tests can help identify patients who are unlikely to gain substantial benefit from chemotherapy and so avoid its side effects.
Treatment for Metastatic Breast Cancer
When breast cancer has spread to distant organs, systemic chemotherapy commonly becomes part of the treatment strategy. The goal in this setting is disease control—slowing cancer growth, relieving symptoms and maintaining quality of life—rather than cure.
Treatment for metastatic disease is often continuous or changed sequentially as the cancer evolves and develops resistance to particular drugs. The treatment team chooses drugs and combinations with an emphasis on balancing effectiveness against likely side effects and the patient’s priorities.
Treatment Goals by Setting
- Neoadjuvant: Shrink tumours before surgery
- Adjuvant: Eliminate microscopic residual disease
- Metastatic: Control spread and manage symptoms
- Curative intent: Achieve complete cancer elimination
- Palliative intent: Improve comfort and extend life
Common Drug Regimens and Protocols
Breast cancer chemotherapy generally uses combinations of drugs rather than single agents. Combining drugs increases the likelihood of destroying cancer cells at different points in their growth and helps to reduce the chance of resistance.
Anthracycline-Based Regimens
Anthracyclines are a long‑standing component of many breast cancer regimens. Doxorubicin and epirubicin are the most frequently used agents in this class; they act by intercalating into DNA and interfering with replication.
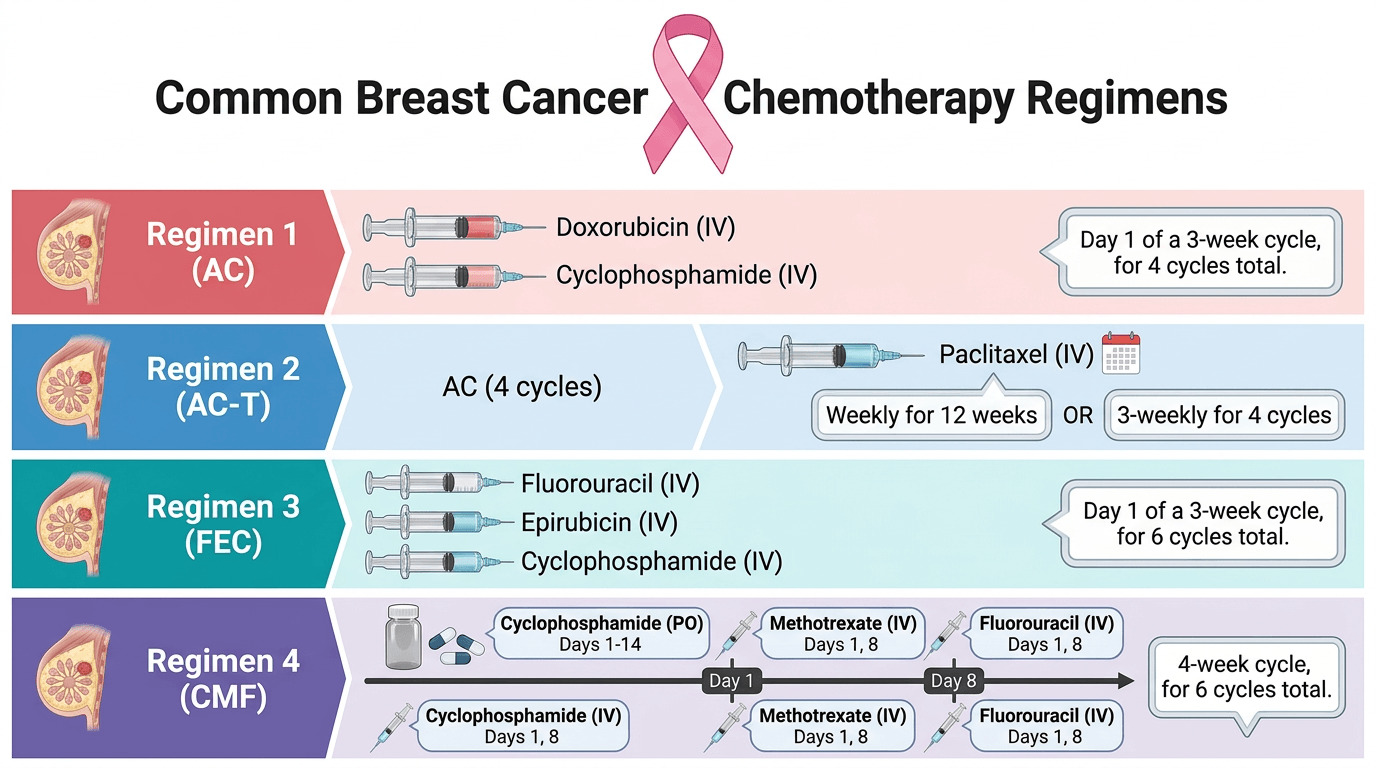
The AC regimen (doxorubicin plus cyclophosphamide) is widely used and typically comprises four to six cycles given about every three weeks as an outpatient. FEC (fluorouracil, epirubicin and cyclophosphamide) is a common UK alternative with similar overall effectiveness; choice between them depends on local practice and individual patient factors.
 Cardiotoxicity is the principal long‑term concern with anthracyclines, particularly at higher cumulative doses. The treatment team monitors heart function with echocardiography or MUGA scans before and during treatment, and may select alternative regimens for patients with pre‑existing cardiac disease.
Cardiotoxicity is the principal long‑term concern with anthracyclines, particularly at higher cumulative doses. The treatment team monitors heart function with echocardiography or MUGA scans before and during treatment, and may select alternative regimens for patients with pre‑existing cardiac disease.
Taxane-Based Protocols
Taxanes (paclitaxel and docetaxel) work by stabilising microtubules and preventing cell division. They are commonly used after or alongside anthracyclines to improve outcomes.
A widely used approach is sequential AC‑T: four cycles of AC followed by weekly paclitaxel for twelve weeks, or alternatively three‑weekly docetaxel. Some centres use concurrent combinations such as TAC (docetaxel, doxorubicin and cyclophosphamide) given every three weeks for six cycles; this shortens overall treatment time but may increase short‑term toxicity.
CMF and Other Combinations
CMF (cyclophosphamide, methotrexate and fluorouracil) predates anthracyclines and taxanes and remains an option for selected patients, for example those with contraindications to modern agents or lower‑risk disease where less intensive therapy is appropriate. CMF tends to have fewer cardiac effects but is generally considered less potent than contemporary regimens.
| Regimen | Drugs Included | Typical Cycles | Administration |
| AC | Doxorubicin, Cyclophosphamide | 4-6 cycles | Every 3 weeks |
| AC-T | AC followed by Paclitaxel | 4 AC + 12 weekly T | Sequential |
| FEC | Fluorouracil, Epirubicin, Cyclophosphamide | 6 cycles | Every 3 weeks |
| TAC | Docetaxel, Doxorubicin, Cyclophosphamide | 6 cycles | Every 3 weeks |
| CMF | Cyclophosphamide, Methotrexate, Fluorouracil | 6 cycles | Every 3-4 weeks |
| TC | Docetaxel, Cyclophosphamide | 4 cycles | Every 3 weeks |
Dose‑Dense and Intensive Approaches
Dose‑dense schedules deliver standard drug doses at shorter intervals (for example every two weeks rather than three) to reduce the time cancer cells have to recover between cycles. Growth factor injections (G‑CSF) are commonly used to maintain blood counts on these accelerated schedules.
Evidence suggests dose‑dense approaches may improve outcomes for certain higher‑risk patients, but they require more frequent hospital visits and closer monitoring. The treatment team discusses the potential benefits and practical implications with each patient when considering this option.
Treatment Duration and Frequency
The expected timeframe for chemotherapy depends on the chosen regimen. Clear information about duration helps people plan work, family and practical support during treatment.
Typical Cycle Lengths and Total Duration
Many regimens use three‑week cycles: treatment on day one followed by a recovery period. Four cycles therefore usually take about twelve weeks, while six cycles extend to roughly eighteen weeks.
Some treatments use weekly schedules, such as paclitaxel given in smaller doses each week for twelve weeks. Although weekly visits are more frequent, individual doses may be better tolerated by some people.
Sequential regimens—for example AC followed by a taxane—naturally extend total treatment time and commonly result in a course lasting five to six months. The treatment team will explain the likely timetable for a specific plan and discuss practical arrangements to support that period.
Factors That May Change the Timeline
Individual tumour response: excellent shrinkage during neoadjuvant therapy confirms effectiveness; progression may prompt an early change of drugs.
Toxicity: low blood counts or other side effects can delay a cycle by a week or more to allow recovery.
Dose adjustments: significant side effects sometimes require dose reductions, which can lengthen the overall treatment period.
Metastatic disease: treatment duration is more variable and often continues until disease progression or unacceptable side effects, with sequential changes of drugs possible over months or years.
Planning consideration: Most people should expect a period of approximately three to six months for standard adjuvant or neoadjuvant chemotherapy. Arranging practical and emotional support in advance helps manage the demands of treatment.
Common Side Effects and Management Strategies
Chemotherapy targets rapidly dividing cells, which includes many cancer cells but also some normal tissues. Knowing the likely side effects and practical ways to manage them helps people feel more prepared and supported during treatment.
Hair Loss and Appearance Changes
Hair loss is often one of the most visible and emotionally difficult effects. Many commonly used regimens cause significant scalp hair loss beginning around two to three weeks after the first cycle; eyebrows, eyelashes and body hair may also thin.
 Hair usually begins to regrow a few months after treatment ends, although initial texture or colour may differ. Scalp cooling systems can reduce hair loss for some drug combinations, particularly taxane‑only schedules, but success varies between individuals.
Hair usually begins to regrow a few months after treatment ends, although initial texture or colour may differ. Scalp cooling systems can reduce hair loss for some drug combinations, particularly taxane‑only schedules, but success varies between individuals.
Practical support includes wigs, scarves and hats; the NHS and charities may be able to help with costs. Offer reassurance that choice is personal and that services exist to help with appearance changes and emotional impact.
Nausea and Digestive Effects
Modern anti‑emetic (anti‑sickness) medications have greatly reduced the burden of nausea. Most patients receive preventive drugs during treatment and take‑home medication for the days immediately afterwards.
Nausea patterns differ by regimen: some people experience early symptoms in the first 48–72 hours, others have delayed nausea several days later. Keeping a symptom diary helps the treatment team tailor anti‑nausea medication effectively.
Dietary tips that commonly help include small, frequent meals, bland low‑fat foods, and maintaining hydration. Cold or room‑temperature foods are often easier to tolerate when taste changes or nausea are present.
Fatigue and Energy Management
Fatigue is among the most common and persistent side effects and can feel different from ordinary tiredness. Energy typically dips after each cycle and may gradually recover before the next treatment.
Practical strategies: prioritise essential tasks, pace activities, and accept help for household and childcare duties.
Activity: gentle exercise such as short walks or light resistance work can improve energy and mood when tolerated.
Rest: schedule short restorative rests and sleep hygiene where possible.
The treatment team can investigate contributing causes such as anaemia, thyroid dysfunction or medication effects and suggest specific measures where appropriate.
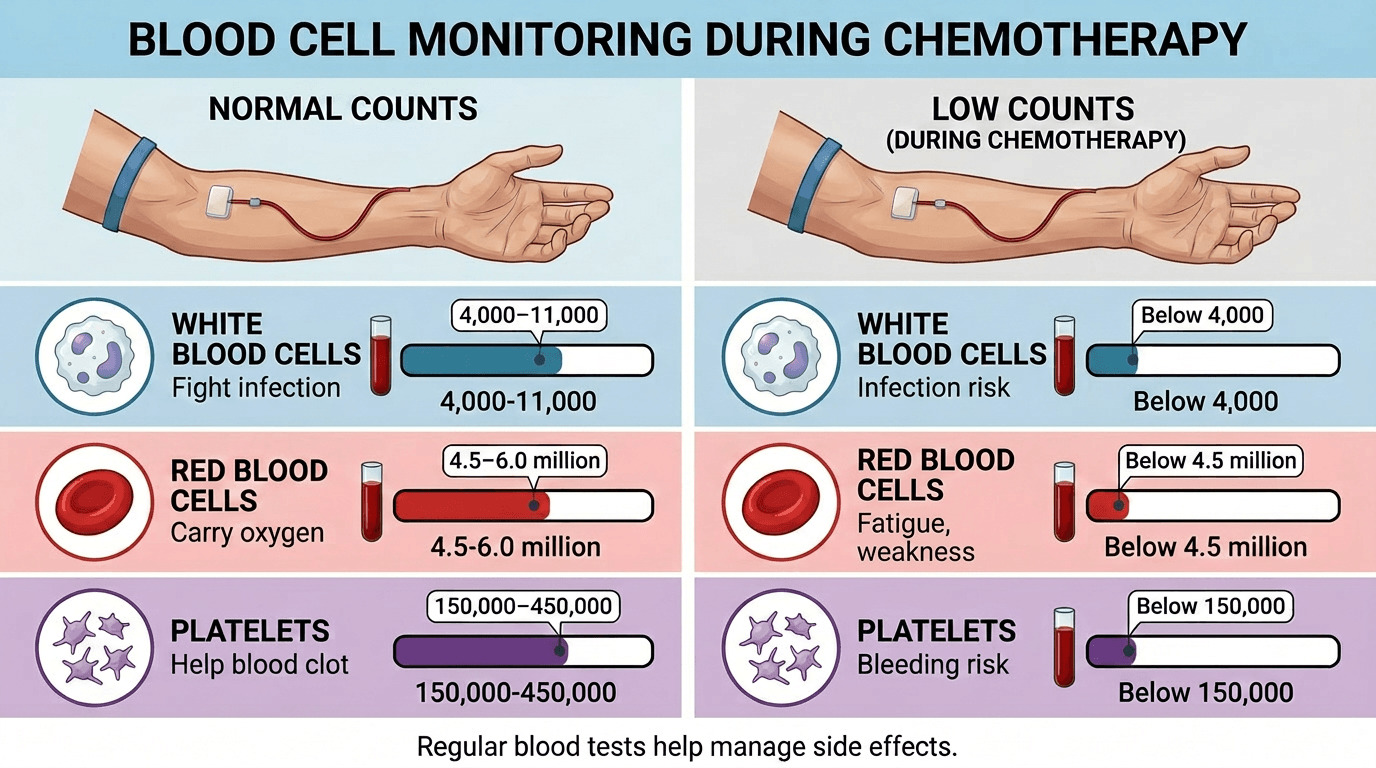
Blood Count Changes and Infection Risk
Chemotherapy commonly reduces white blood cells, red cells and platelets. Counts typically fall to their lowest point (nadir) seven to fourteen days after a cycle; regular blood tests guide safe timing for each dose.
Low white cell counts increase infection risk. If fever occurs during treatment, follow local instructions promptly—many centres advise urgent assessment and treatment. Some trusts use a fever threshold of 37.5°C, while others use 38.0°C; follow the guidance provided by the treatment team or oncology unit.
Preventive measures include good hand hygiene, avoiding close contact with unwell people when counts are low, and promptly reporting symptoms to the oncology helpline. Growth factor injections (G‑CSF) are used in some regimens or with dose‑dense schedules to reduce the duration of low white cell counts.
Peripheral Neuropathy
Some drugs, particularly taxanes and certain others, can cause peripheral neuropathy — numbness, tingling or pain in the hands and feet. Symptoms often start in the fingertips and toes and may progress with cumulative exposure.
Mild neuropathy frequently improves after treatment, though recovery can take months. If neuropathy affects daily activities, the treatment team may consider dose reduction or changing agents. Occupational therapy offers practical strategies and aids to preserve independence.
Mouth Sores and Taste Changes
Certain drugs cause mucositis — inflammation and sores in the mouth and throat — which can make eating and drinking uncomfortable. Good oral care is important: gentle brushing, alcohol‑free mouthwashes, and simple saline rinses often help. The oncology team can prescribe specific mouthwashes or pain relief if needed.
Taste changes are common and may make food taste metallic, overly sweet or bland. Experimenting with different flavours, textures and temperatures helps identify acceptable options until taste returns to normal.
Cognitive Changes
Some people report problems with memory, concentration and mental processing during or after chemotherapy, often called “chemobrain.” These effects are usually mild and improve over time, though they can be distressing.
Practical strategies include using reminders and planners, breaking tasks into smaller steps, and reducing multitasking. Cognitive rehabilitation programmes or occupational therapy can assist where difficulties are significant.
Access Specialist Support Throughout Your Treatment
Navigating the physical and emotional challenges of chemotherapy requires comprehensive support. Specialist services provide personalized advice on managing appearance changes, maintaining comfort, and addressing the practical aspects of treatment. Professional guidance helps patients feel more confident and supported throughout their cancer journey.
Considerations for Different Breast Cancer Types
Breast cancer comprises a range of biological subtypes that require tailored systemic treatments. The tumour’s characteristics determine which chemotherapy agents or additional targeted therapies are appropriate.
Triple Negative Breast Cancer
Triple‑negative tumours lack oestrogen and progesterone receptors and do not overexpress HER2, so endocrine or HER2‑targeted drugs are not effective. Chemotherapy therefore remains the principal systemic treatment option for this subtype.
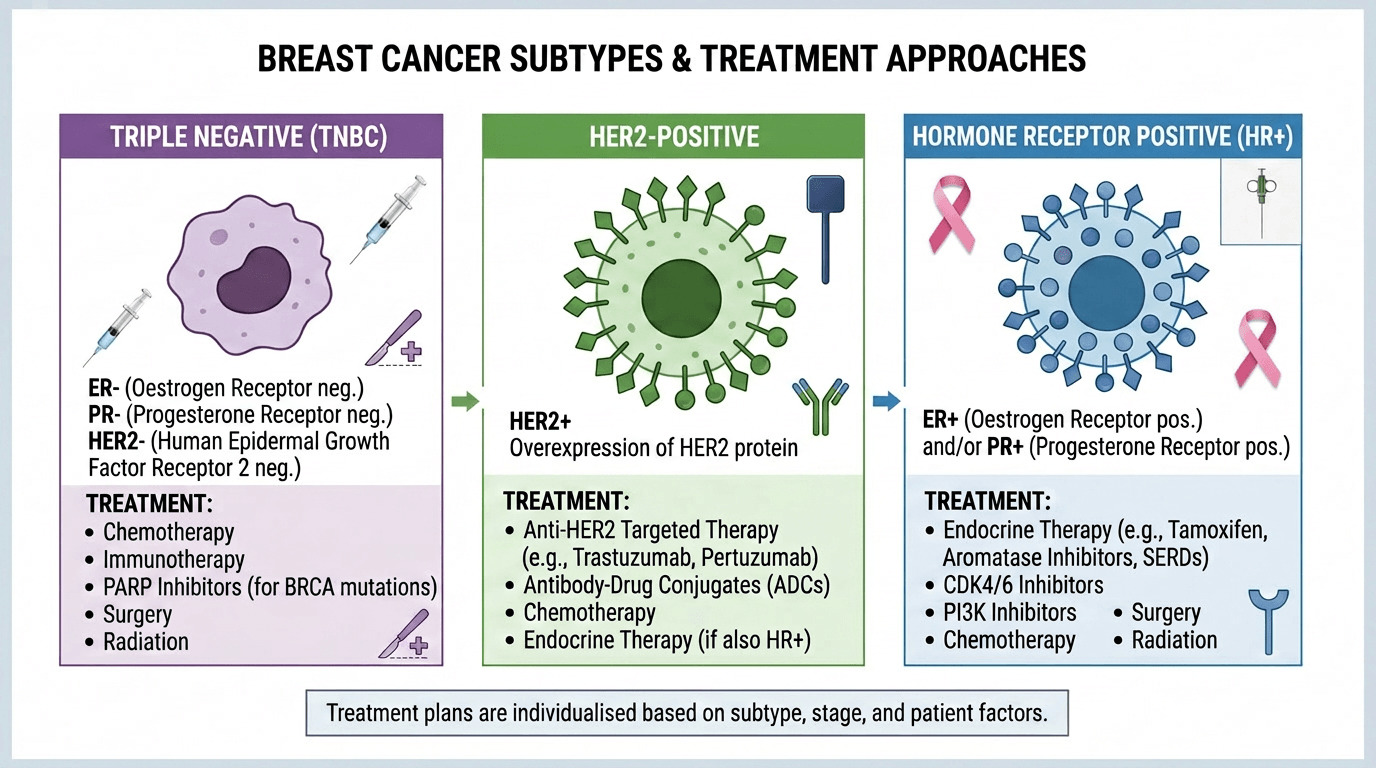 Triple‑negative cancers often respond well initially to chemotherapy, and neoadjuvant approaches are commonly used to assess response. Regimens usually include anthracyclines and taxanes, and selected patients may receive additional platinum drugs such as carboplatin.
Triple‑negative cancers often respond well initially to chemotherapy, and neoadjuvant approaches are commonly used to assess response. Regimens usually include anthracyclines and taxanes, and selected patients may receive additional platinum drugs such as carboplatin.
In selected cases, immunotherapy has been added to chemotherapy where specific biomarkers indicate likely benefit; this is determined by the treatment team and specialist testing. When to consider chemotherapy: typically recommended for most patients with triple‑negative disease because alternative targeted options are limited.
HER2-Positive Breast Cancer
HER2‑positive tumours overexpress the HER2 protein, which promotes tumour growth. The development of HER2‑targeted agents has substantially improved outcomes for this group when given alongside chemotherapy.
Standard practice usually combines chemotherapy with HER2‑targeted drugs such as trastuzumab (Herceptin) and pertuzumab, with trastuzumab commonly continued to complete about one year of therapy. Cardiac monitoring is important because trastuzumab and some anthracyclines carry a risk of cardiotoxicity; the treatment team arranges regular heart checks and adapts treatment for patients with cardiac concerns.
When to consider chemotherapy: generally advised for most HER2‑positive cancers in combination with HER2‑directed therapy, tailored to individual risk and cardiac status.
Hormone Receptor Positive Breast Cancer
The majority of breast cancers express oestrogen and/or progesterone receptors. For many of these tumours, hormone therapy forms the backbone of systemic treatment; the need for chemotherapy depends on additional factors.
Genomic tests such as Oncotype DX or Prosigna can help estimate the likely benefit of adding chemotherapy in early‑stage, hormone receptor positive, HER2‑negative disease. These assays produce a recurrence score that assists the treatment team in balancing potential benefit against the side effects of chemotherapy.
When to consider chemotherapy: recommended when clinical and genomic factors together indicate a meaningful reduction in recurrence risk; otherwise, many patients do well with endocrine therapy alone, often continued for five to ten years.
Early Stage Versus Advanced Disease
In early stage breast cancer confined to the breast and nearby lymph nodes, treatment aims for cure and chemotherapy intensity may reflect this curative intent. In advanced or metastatic disease the objective shifts to prolonging life and preserving quality of life; drug choice often favours agents or combinations with better tolerability and sequencing as resistance develops.
Preparing for Treatment and Building Support Systems
Practical preparation and emotional support make chemotherapy more manageable. Advance planning for tests, logistics and wellbeing reduces stress and helps maintain stability throughout treatment.
Pre-Treatment Assessments and Planning
Before chemotherapy starts, the treatment team arranges baseline assessments to ensure safety. These typically include blood tests to check blood counts, liver and kidney function, and, when indicated, tumour markers. Cardiac assessment (echocardiogram or MUGA) is performed if cardiotoxic drugs are planned.
Discuss fertility preservation early with the oncology team, since many chemotherapy drugs can affect reproductive capacity. Options such as egg or embryo freezing may be offered, but time‑sensitive decisions are sometimes required.
A dental check is advisable before treatment, as dental problems can worsen during chemotherapy when infection risk and healing may be affected.
Practical Arrangements
Planning practical matters reduces day‑to‑day pressure. Consider arranging:
Work adjustments – discuss flexible hours, phased return or medical leave with employers and seek human resources or occupational health support.
Childcare and household help – organise reliable assistance for the first few days after each cycle when fatigue is often greatest.
Transport – plan how to travel to appointments and whether a driver is available; explore patient transport schemes if needed.

Emotional and Psychological Support
The psychological impact of cancer can be profound. Early access to support helps develop coping strategies and reduces isolation. Many centres offer counselling, psycho‑oncology services or support groups; ask the treatment team for local resources and referrals.
Peer support often provides practical tips and emotional validation. Hospitals, charities and online communities run groups where experiences and coping strategies are shared. It may take time to find the right support network; trying different options can help identify what fits best.
Family and friends usually want to help but may be unsure how. Be specific about needs—meals, transport, childcare or companionship—and accept offers of practical assistance.
Financial Considerations
Cancer treatment often brings extra costs despite NHS care, including travel, parking and items such as wigs. Hospital social workers and Macmillan benefits advisers can help identify entitlements and complete benefit applications.
Benefits such as Personal Independence Payment or Employment and Support Allowance may be relevant; professional advice makes applications easier. Charities also offer grants for specific needs. For regular prescriptions, a Prescription Prepayment Certificate can reduce medication costs during treatment.
Monitoring During Treatment and Follow-Up Care
Regular monitoring during chemotherapy ensures safety and allows early management of complications. After treatment finishes, follow‑up care focuses on detecting recurrence where appropriate and addressing long‑term effects to optimise recovery and quality of life.
Surveillance During Active Treatment
Key monitoring during active chemotherapy includes:
Blood tests before each cycle to check white cells, red cells, platelets and liver and kidney function — these results determine whether it is safe to proceed.
Clinical review at each visit to discuss symptoms and side effects so supportive medicines or adjustments can be made promptly.
Imaging where indicated — for example during neoadjuvant treatment to assess tumour shrinkage, or in metastatic disease to monitor response and guide changes in therapy.
Open communication with the treatment team about any new symptoms, however small they may seem, enables timely intervention and safer treatment delivery.
Completion Assessment and Surgical Planning
Following neoadjuvant chemotherapy, repeat imaging assesses residual tumour size and helps plan surgery. When substantial shrinkage has occurred, markers placed at diagnosis assist surgeons in locating the original tumour site. The interval to surgery varies by protocol and individual recovery; the treatment team balances adequate healing with avoiding unnecessary delay.
Long-Term Follow-Up
After completion of all planned treatment, routine follow‑up typically begins with visits every three to six months and then spaces out to annual appointments after several years, though exact schedules vary between centres. These reviews focus on:
Clinical examination and discussion of any new symptoms
Annual mammography of the treated breast and the opposite breast
Monitoring and management of late effects such as cardiac issues (after cardiotoxic drugs), persistent neuropathy, cognitive changes or fatigue
Routine whole‑body imaging for asymptomatic patients is not generally recommended because it has not been shown to improve survival; local guidance varies and the treatment team will advise the appropriate surveillance schedule for each person.
Those prescribed long‑term hormone therapy require ongoing review for side effects and adherence support. The transition from intensive treatment to maintenance and survivorship can be challenging; survivorship programmes and supportive services help address both physical and psychological needs.
Lifestyle Factors and Wellness During Treatment
Supporting the body through chemotherapy goes beyond managing side effects. Nutrition, physical activity and wider wellbeing measures contribute to treatment tolerance, recovery and overall quality of life.
Nutrition and Dietary Considerations
Maintaining adequate nutrition helps sustain strength and supports healing. Appetite changes, taste alterations and nausea commonly make eating harder, so focus on nutrient‑dense choices when appetite allows.
Protein: include a source of protein at each meal and snack—lean meat, fish, eggs, dairy, beans or nuts. Fortified drinks can help when solid food intake is limited.
Hydration: keep fluids up, especially with diarrhoea or vomiting—water, diluted juice, herbal tea and broths all help.
Food safety: avoid unpasteurised dairy, raw or undercooked meats and eggs, and unwashed produce when white cell counts are low.
Small, frequent meals and bland, low‑fat options often sit better than large or spicy meals. Experiment with flavours and temperatures to find what is most tolerable during treatment.
Physical Activity and Exercise
Exercise during chemotherapy may seem difficult, but gentle activity has consistent benefits: reduced fatigue, preserved muscle strength, improved mood and better overall wellbeing. Adapt activity to daily energy levels.
On good days: aim for longer walks, gentle yoga or light resistance training.
On difficult days: short walks or simple mobility exercises still provide benefit.
Strength: light resistance work with bands or small weights helps counteract muscle loss.
 Many cancer centres offer specialised exercise programmes and physiotherapy advice; discuss plans with the treatment team before starting a new regimen to ensure safety and suitability.
Many cancer centres offer specialised exercise programmes and physiotherapy advice; discuss plans with the treatment team before starting a new regimen to ensure safety and suitability.
Stress Management and Mental Wellbeing
Deliberate strategies to manage stress protect mental health during treatment. Mindfulness, brief daily relaxation exercises and paced breathing can reduce anxiety and improve emotional regulation.
Mind‑body: mindfulness or gentle yoga can help with anxiety and sleep.
Creative outlets: art, music or writing provide distraction and a sense of accomplishment.
Social contact: maintaining connections by phone, video or short visits combats isolation and supports coping.
Professional psychological support and counselling are available through many cancer centres; ask the treatment team for referrals if needed.
Complementary Approaches
Some people find complementary therapies helpful alongside conventional treatment. Acupuncture may offer relief for nausea or neuropathy in selected cases, and massage can reduce stress—ensure practitioners understand oncology‑specific precautions.
Herbal supplements can interact with chemotherapy and should only be used after discussion with the oncology team. Approaches such as aromatherapy, music therapy and reflexology typically pose low risk and may provide comfort, but they do not replace medical treatment.
Recent Advances and Future Directions
The landscape of breast cancer chemotherapy is evolving. New drugs, improved supportive care and more personalised approaches are increasing effectiveness while reducing unnecessary treatment burden.
Genomic Testing and Treatment Personalization
Genomic assays increasingly inform decisions, especially for hormone receptor positive disease. These tests analyse tumour gene expression to estimate recurrence risk and the likely benefit of adding chemotherapy to other treatments.
Oncotype DX is widely used in UK practice to generate a recurrence score that helps the treatment team discuss the balance of benefits and harms for an individual. Low scores suggest limited benefit from chemotherapy, while higher scores indicate greater potential benefit; results in the intermediate range require careful discussion of other clinical factors.
Overall, genomic testing has reduced unnecessary chemotherapy for many people with early‑stage, hormone receptor positive breast cancer by identifying those unlikely to gain meaningful benefit.
Novel Drug Combinations and Sequencing
Ongoing research evaluates optimal combinations and sequencing of systemic drugs. Adding platinum agents such as carboplatin to standard regimens appears beneficial in some triple‑negative cancers, with investigation continuing into which subgroups gain most advantage.
Antibody–drug conjugates are a notable advance: these link cytotoxic drugs to antibodies that target specific proteins on cancer cells, delivering treatment more selectively and limiting exposure to normal tissues. Agents such as trastuzumab deruxtecan and sacituzumab govitecan have shown meaningful activity in selected, previously treated metastatic settings under specialist supervision.
Improved Supportive Care
Better supportive medications reduce treatment side effects and help people complete planned chemotherapy. Advances include more effective anti‑nausea regimens, improved growth factors and enhanced symptom management strategies.
Scalp cooling technology continues to improve and may reduce hair loss for some patients, although suitability depends on the drugs used and individual factors. Psycho‑oncology services are increasingly integrated into routine care, recognising the importance of mental health alongside physical treatment.
What this means for patients: treatment is becoming more precise — targeted drugs and better tests allow the treatment team to offer options that match the cancer’s biology while improving tolerability and preserving quality of life.
Making Informed Treatment Decisions
Choosing whether to have chemotherapy requires weighing likely benefits against probable side effects and the effect on quality of life. Good decisions combine accurate medical information with clear consideration of personal priorities and life circumstances.
Understanding Treatment Goals
Clarifying the objective—cure, reduced recurrence risk, symptom control or life extension—helps put trade‑offs into perspective. When the goal is curative, accepting greater short‑term toxicity may be justified by a substantial long‑term benefit; the balance is different when the aim is symptom control in advanced disease.
Discuss with the treatment team the expected absolute benefit of chemotherapy (for example how much it reduces the chance of recurrence in percentage points), not only relative figures. A simple illustration: reducing recurrence from 20% to 10% is a 50% relative reduction but an absolute reduction of 10 percentage points, meaning ten people would be treated to prevent one recurrence. This “number needed to treat” helps frame the likely population benefit alongside individual impact.
Shared Decision‑Making
The best decisions are collaborative. Clinicians provide evidence about likely outcomes, side effects and uncertainties. People bring their own values, priorities and tolerance for risk. Together these perspectives produce a plan that fits the individual.
Decision aids and summary sheets can structure consultations and make complex information easier to compare. Consider bringing a written list of priorities or questions to appointments to ensure concerns are addressed.
Helpful questions to ask the team: What absolute benefit do you expect from chemotherapy for my cancer? What are the most likely side effects and how will they be managed? How will treatment affect daily life and work? Are there reasonable alternatives?
Ask about practicalities: likely duration, frequency of visits, and support services available.
For decisions where reasonable options exist, there is no single correct choice—what matters is that the chosen path aligns with the person’s goals and values.
Second Opinions and Additional Perspectives
Seeking a second opinion is appropriate for complex cases or when uncertainty remains. Most oncologists support additional perspectives, and specialist centres may offer expertise for rare subtypes or unusual scenarios. The primary clinician can usually facilitate referrals.
While additional opinions can increase confidence or present alternatives, repeatedly seeking different viewpoints to avoid a decision may delay treatment; at some point a choice is needed based on the best available information and trusted clinical advice.
Frequently Asked Questions About Breast Cancer Chemotherapy
How long does chemotherapy for breast cancer typically last?
Standard chemotherapy courses commonly run three to six months, depending on the regimen. Many protocols use two‑ or three‑week cycles; four cycles therefore often take about twelve weeks, while sequential AC followed by a taxane may extend to five or six months. Weekly schedules, for example paclitaxel given weekly for twelve doses, also span roughly three months. The exact duration depends on cancer type, stage and the specific drugs chosen by the treatment team.
Will chemotherapy definitely cause hair loss?
Many breast cancer chemotherapy regimens cause significant hair loss, but the extent varies by drug. Anthracyclines and taxanes often produce scalp hair loss beginning two to three weeks after the first cycle; body hair, eyebrows and eyelashes may also thin. Some regimens cause only thinning. Scalp cooling can reduce hair loss for some people, particularly with taxane‑only schedules, although effectiveness varies.
What are the most common drugs used for breast cancer?
Common agents include doxorubicin and epirubicin (anthracyclines), paclitaxel and docetaxel (taxanes), and cyclophosphamide. These are combined in regimens such as AC (doxorubicin + cyclophosphamide), FEC (fluorouracil, epirubicin, cyclophosphamide) or TAC (docetaxel, doxorubicin, cyclophosphamide). Carboplatin is increasingly used in some triple‑negative cases. HER2‑positive cancers receive chemotherapy alongside HER2‑targeted drugs.
Can chemotherapy be given as tablets rather than through a drip?
Most standard adjuvant and neoadjuvant regimens are given intravenously to ensure accurate dosing and immediate management of reactions. Some agents, such as capecitabine, are oral and may be used in metastatic disease or specific protocols. Cyclophosphamide can sometimes be administered orally. The route depends on the chosen drugs and the clinical setting.
How soon after surgery does chemotherapy typically start?
Adjuvant chemotherapy usually begins three to six weeks after surgery to allow wounds to heal while avoiding undue delay in systemic treatment. Exact timing depends on recovery, wound healing and coordination with surgical teams; port placement or other procedures may occur beforehand if required.
Are there alternatives to chemotherapy for breast cancer?
Alternatives depend on tumour biology. Hormone receptor positive cancers may be managed with endocrine therapy alone when genomic testing indicates low recurrence risk. HER2‑positive cancers require HER2‑targeted drugs alongside or instead of chemotherapy in certain situations. Radiation treats local disease but does not address systemic spread. The treatment team determines which options are effective for each cancer type.
Where can I find support during chemotherapy?
Support is available from hospital specialist nurses, counsellors and local support groups, as well as national charities such as Breast Cancer Now, Cancer Research UK and Macmillan. Peer support groups and online communities can provide practical advice and emotional support. Specialist services like Donna Forte offer personalised advice on managing practical and emotional challenges. NHS Patient Advice and Liaison Services (PALS) can also signpost local resources.
Will nausea be constant throughout chemotherapy?
Modern anti‑nausea medications have greatly reduced persistent sickness. Most people do not experience constant nausea; symptoms are often worst in the first few days after a cycle or may appear later. Preventive medications before treatment and take‑home prescriptions for subsequent days typically control symptoms, and the regimen can be adjusted if needed.
Can I work during chemotherapy treatment?
Many people continue working, often with adjustments. Feasibility depends on job demands, treatment intensity and individual side effects. Flexible hours, reduced duties or temporary leave can help. Discuss options with employers and the treatment team to find a sustainable plan that balances work and recovery.
What happens if side effects become too severe?
The treatment team can modify therapy if side effects are unmanageable. Options include dose reductions, treatment delays, switching regimens or enhanced supportive care such as growth factors and alternative anti‑nausea drugs. Severe complications may rarely require stopping chemotherapy; open communication about side effects enables timely adjustments to maintain safety and quality of life.
How will I know if chemotherapy is working?
Assessment depends on the treatment setting. For neoadjuvant therapy, clinical examination and imaging track tumour shrinkage and guide surgical planning. After adjuvant treatment there is no immediate test of success; benefit is measured over time by reduced recurrence. In metastatic disease, regular scans and sometimes tumour markers assess response and guide further treatment decisions. The treatment team will explain the monitoring plan for each individual case.
Moving Forward With Confidence
Chemotherapy is often a key element of comprehensive breast cancer care. Clear information about how treatment works, likely side effects and available sources of support helps people and their families navigate this period with greater confidence and preparation.
 Treatment continues to improve: better drugs, enhanced supportive care and more personalised approaches based on tumour biology mean more effective therapy with less unnecessary burden. Genomic testing increasingly helps the treatment team identify who will most benefit from chemotherapy and who may safely avoid it, reducing exposure to side effects.
Treatment continues to improve: better drugs, enhanced supportive care and more personalised approaches based on tumour biology mean more effective therapy with less unnecessary burden. Genomic testing increasingly helps the treatment team identify who will most benefit from chemotherapy and who may safely avoid it, reducing exposure to side effects.
Decisions about therapy combine clinical evidence with personal values. Clinicians offer expertise about likely outcomes and risks; patients contribute knowledge of their priorities and what matters most in daily life. Together these perspectives produce a plan aligned with individual goals.
Support comes from many sources—medical teams, family and friends, peer groups and specialist services such as Donna Forte. While chemotherapy is challenging, it is finite and manageable for most people. Each completed cycle is progress towards improved long‑term health and the possibility of many years ahead.
Disclaimer: This guide is for informational purposes only and not a substitute for professional medical advice. Always consult your own doctor or oncology team before making any health decisions.